Are future psychiatric treatments doomed?
Be careful what you ask for…you just might get it.
NEI Blog
Neuroscience Education Institute
by Stephen Stahl
August 23, 2011
Nobody likes drug companies these days. Worse than tobacco companies and big oil companies! Supposedly they have ruined CME and have corrupted psychiatric experts as consultants, lecturers and research grant recipients! Drug companies only engage in expensive patent extension gimmickry and offer no true innovations! Let’s criminalize the marketing of psychiatric drugs, levy billions in fines to Pharma, force out their CEOs and even make them and their Pharma collaborators take the “perp walk” on their way to court in chains and orange jumpsuits and in front of the cameras! Get out of our professional societies! Get out of our journals! Get out of our medical centers! Good riddance!!!……the anti-psychiatry community, lights up the antipsychiatry blogs [e.g., Carlat] who attract the Pharmascolds, scientologists and antimedication crowd who believe either there is no such thing as mental illness, that medication should not be used, or both. Did you know that psychiatric illnesses are pure inventions of Pharma and their experts to treat patients that do not exist with drugs that are dangerous and do not work with the purpose only of profiting themselves? Stop the profits! Make mental illness go away by legislation and committee! Treat human mental suffering with love and peace and all will be well! Who needs mental health professionals and their diabolical drugs anyway?…
I am blogging today from Paris at the ECNP [European College of Neuropsychopharmacology] meeting, having attended the Royal Society of Medicine meeting outside of London last week to discuss the future of new drug development in psychiatry, paid by the taxpayers of the UK and charities, not Pharma. This meeting involved US colleagues Tom Insel [head of the National Institute of Mental Health], David Kupfer [head of DSM V rewrite], and several academic experts and industry executives from the US and the UK and was covered by the BBC and a report of it aired on UK television…
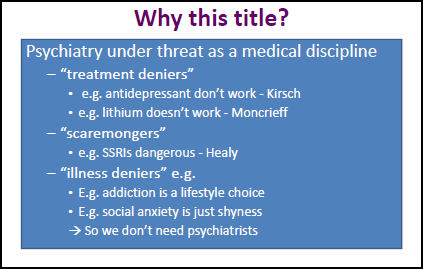
At a meeting of the Royal College of Psychiatrists in Brighton in June 2011, Dave Nutt, a professor of psychiatry at Imperial College London issued a call to arms to his audience at a plenary lecture to defend psychiatry which in Dave’s view meant defending psychopharmacology. On a slide entitled ‘No Psychiatry Without Psychopharmacology’ he outlined the threats from treatment deniers like Irving Kirsch and Joanna Moncrieff whom he claimed argued drugs don’t work. Psychiatry is also apparently threatened by illness deniers who claim that addiction or shyness are just lifestyle options. Then labeling and libeling me a Scaremongerer, he claimed psychiatry was threatened by me. The first point to note is that I was not held to deny the reality of illness nor held to say that treatments don’t work.As regards the risks of drugs, pharmaceutical companies are quick to sue people who claim that treatments have risks if they cannot back up their claims with evidence. As we have seen in the first post in this series almost everything I write or say at meetings is scrutinized with a view to suing me. Calling someone a Scaremongerer, as a matter of logic, should be all but an oxymoron – such a beast cannot exist. The only risks that can be mongered are ones that are real. If these risks are real, should they be regarded as scares? If the argument is that it is fear that is being mongered, pharmaceutical companies monger fear the whole time. Leave your child’s depression untreated and she will grow up to be alcoholic, a drug abuser, will have a failed career and marriage and ultimately commit suicide. Leaving your anxiety or depression untreated while pregnant and your child is likely to be born with a birth defect. If medicine is going to save itself, if it is going to remain a profession, it is time to embrace the duties given it in 1951 and again in 1962 when drugs were made available on prescription-only. Doctors warn people about the risks of over-the-counter products – like patent medicines or tobacco. Prescription-only medicines are prescription only precisely because they are riskier than over-the-counter drugs. If they are no riskier than alcohol or nicotine, which people can manage on their own, why have them on prescription-only. Doctors are there to quarry information out of pharmaceutical companies about these risks – not to be a risk-denying conduit for drugs.
Dave, who I used to think of as a friend or at least a colleague, has form in this area. He has instigated investigations of me by the General Medical Council, aimed it would seem at getting me debarred from practice. After this lecture, I sent an email asking for the slide branding me a scaremonger – it’s one to treasure – but he didn’t respond. Dave has another role which is agitating on behalf of the pharmaceutical industry – making regulations less onerous and the environment more company friendly so companies don’t move jobs elsewhere… The thrust of a series of recent posts here … is that if doctors cannot be identified as the people who know about the risks of drugs, they are likely to go out of business. They should be scaremongerers in other words.
Now is the time for doctors to come out of the closet. We urgently need to develop Scaremonger Pride to match Black, Gay and Mad Pride. I’m open to nominations for a Dave Nutt Prize for most effective Scaremongering of the Year for 2011 and would urge everyone to keep track of possible nominees for 2012. You can nominate the person who in your opinion did the most to alert others to a hitherto unknown or poorly recognized substantial risk from some treatment. Anne-Marie or Rosie Meysenburg would be good candidates for 2011.
 Dr. Healy is no stranger to being discounted because of his determination to talk about the truth of Akathisia and suicidality in some patients on SSRIs – something he ran across as a clinician early in his career as a biological psychiatrist. In 2001, he lost a job in Toronto in a now famous encounter with the infamous Dr. Charlie Nemeroff after lecturing on his findings [before that became cool!…]. In the contemporary version, Dr. Nutt can’t bring off discounting Healy as part of some fringe group [a treatment denier or an illness denier], so he gives Healy his own category [scaremonger] implying that Healy has some crazy motive to invoke fear in others. Dr. Healy uses this moniker, scaremonger, to point out the essential tragedy in this whole story. Warning patients accurately about the dangers of medications and conveying their true efficacy is, in fact, the delegated job of physicians. It’s the reason we were given prescribing privileges in the first place! Healy’s point highlights the absurdity of Nutt’s next slide:
Dr. Healy is no stranger to being discounted because of his determination to talk about the truth of Akathisia and suicidality in some patients on SSRIs – something he ran across as a clinician early in his career as a biological psychiatrist. In 2001, he lost a job in Toronto in a now famous encounter with the infamous Dr. Charlie Nemeroff after lecturing on his findings [before that became cool!…]. In the contemporary version, Dr. Nutt can’t bring off discounting Healy as part of some fringe group [a treatment denier or an illness denier], so he gives Healy his own category [scaremonger] implying that Healy has some crazy motive to invoke fear in others. Dr. Healy uses this moniker, scaremonger, to point out the essential tragedy in this whole story. Warning patients accurately about the dangers of medications and conveying their true efficacy is, in fact, the delegated job of physicians. It’s the reason we were given prescribing privileges in the first place! Healy’s point highlights the absurdity of Nutt’s next slide:
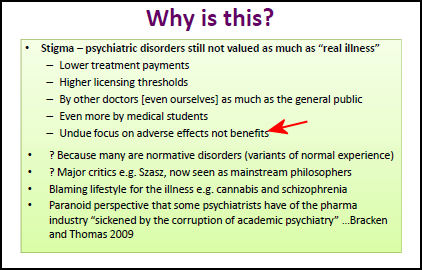
It is the point that Dr. Healy fleshes out in his recent book, Pharmageddon. And Dr. Nutt has things backwards. What has and will put "Psychiatry under threat as a Medical Discipline" is actually the "undue focus on … benefits" – AKA lying…
There is an irony in this story. Dr. Nutt himself was a truth-sayer. In 2008, he became Chairman of the Advisory Council on the Misuse of Drugs. He was an outspoken advocate for basing the laws about street drugs on their true evidence-based dangers – publishing this graph in The Lancet:

In 2009, Dr. Nutt was fired from this appointment because of his own truth-saying about Street Drugs [and one has to wonder where the prescription medications Nutt both promotes and defends would fall on his own graph].
Don’t hold us accountable or else!
No patient should leave with a prescription for a drug without being informed of the risks, including paradoxical reactions. With hallucinogenic street drugs, a subculture was formed to describe good and bad affects and to “babysit” people while they were “tripping”. Many mental health professionals are giving people drugs that effect them all day every day with little warning. Having the information that a drug might have profound effects that are NOT desirable would give the patient fair warning, so that if that bad reaction did occur, the patient would be more likely to recognize it as aberrational and call the doctor so that he can do something about the effects of the drug he/she prescribed.
Even when patients know they’ll have a bad reaction to a drug, refusal to take something the doctor prescribes is often seen as wanting to be manic. If you tell him you remember that one because it made you ANGRY you’re not making any sense to them. Drugs good. Patients bad.
Wanting to be considered an unquestioned authority while treating your patients like your very own red-headed step-children is being a bully. It’s no surprise to me that a lot of psychiatrists turn on other psychiatrists who question their authority.
Dr. Healy advocates for brain damage by ways of an invisible knife, a knife of electricity as a solution to problems of the mind.
It is all damage to the brain.
Doctors don’t jail their patients. Psychiatry does.
Doctors honor the “First, do no harm” part of being a doctor. Psychiatrists do hurt the physical brain of their patients. Psych patients have up to a 25 year shorter life span.
If all humans are sinners, does my psychiatrist have less sin ( in order to help another) than I?
The psychiatrist is working for the patient, or for the money? The patient isn’t paying you say? The Government is paying?
Sweet Dreams Eurythmics
Some of them want to use you
Some of them want to get used by you
Some of them want to abuse you
Some of them want to be abused
Some of them want to help you (psychiatrists)
some of them want to be helped (patients)
Caffeine is not on the “dependance vs physical harm” chart..
I don’t get it. Psychiatry has about 3 dozen drugs to mix and match. If there’s nothing wrong with these drugs, why will it wither and die if it doesn’t have new drugs? Is there something about drug novelty that is necessary to the practice of psychiatry?
(Dr. Carlat gets another good laugh. Calling him antipsychiatry is like calling Olympia Snow a Marxist.)
Attacking the truthsayers goes both ways. Some people have benefited from ECT when nothing else helped them. McManus sums it up here
Ironically, ECT’s worst enemy has been the psychiatric profession. The over-use of the treatment during the forties and fifties and sixties, often against the patient’s will, under primitive conditions, and on populations upon whom the procedure conferred no benefit, gave rise to strong opposition. Part of the backlash came from the new antipsychiatry movement which got its start from patients who had been abused by ECT and inhumane institution-based practices. The movement found ready allies in other sixties-era groups pressing for political and social reform.
But there was still the persistent problem of memory loss to contend with. Psychiatry did not help its own cause by repeatedly down-playing and even denying this disturbing invasion to the brain’s hard drive. Ludicrously, psychiatrists picked fights with patients who uncooperatively reported they could no longer remember their own kids’ birthdays. Clinical evidence, anecdotal or otherwise, was difficult to come by, as few clinicians even bothered to follow up on their patients.
http://www.mcmanweb.com/ect.html
My favorite psychiatrist and my neurologist both earned my respect by stating plainly that much is not known about the conditions they are trying to treat, and a lot of the work they do is trial and error and a game of elimination. A doctor in psychiatry who appears to think he’s the expert’s expert on all matters psychological including the mind and life of a patient is an arrogant buffoon.
A doctor who doesn’t admit even to himself the dangers of a drug or procedure is a threat to his patients and his profession. Having wisdom would require a p-doc to examine all charges against the use of any psychoactive drug or procedure with as much objectivity as he/she can muster with the good of the patient and community foremost in his/her mind.
We don’t have to understand everything to know that a procedure or drug can be beneficial, anymore than we have to understand the science of gravity to stick to the ground; but that lack of knowledge, in the mind of a medical doctor should lead to humility.
Did you take a gander at the stigma slide? It’s all about psychiatry suffering from stigma. Patients aren’t even mentioned. And who inflicts this awful stigma?
Szasz gets a mention.
Orwell is spinning.
Thanks Mickey. A great read!
Altostrata your question hit me like a thunder.
I have been thinking exactly that question and this is my conclusion:
The brain will always “adapt to being exposed” to psychotropics. So the effect of a novel psychotropic will never be static. As the population get exposed to a psychotropic and the brain adapt, it will end up losing the magic effect. So to survive we need a magic (read different receptor binding) pill to keep the interest in psychiatry. No only from the patients point of view, but the industry need to develop “new” read different receptor binding molecules to create the whao effect that will take some time of exposure to be lost.
As an old psychiatrist told me once, if the patient is not stable with good compliance to medication and we see even more frequent relapses, the drug is doing something wrong or the patient is adapting by genetically re-inforcing the expression of the disease.
By the way medications do work until the brain adapt and them, they can not do what they were doing initially.
We see this as the disease progress:
Schizophrenia then Schizoaffective disorder;
Major Depressive Disorder then Bipolar;
Bipolar then ADD or viceversa;
After chronic exposure they do not work at all, but they can not be stop because the patients rebound (withdrawal) from the adaptation that is ensuing due to chronic exposure.
Possible solution: -Do not treat patients chronically with psychotropics, exactly the opposite of what we do.
-If you switch or discontinue the psychotropic, before you throw a new diagnosis (exactly what we do) please rule out rebound and do the discontinuation differently.
An excellent point, well made. It’s actually my take on Robert Whitaker’s findings in other cultures where Schizophrenic patients are only treated acutely. My own experience is that it’s not as easy, because both patient and family have to accept the possibility of relapses, particularly early on. But I think it’s what we would do in the best of all possible worlds. Use medications intermittently, sparingly, and keep much closer tabs on people.
Giovanni Fava believes the nervous system naturally accommodates to medication to maintain homeostasis (until, possibly, it is overwhelmed by excessive or chronic medication). Eventually “oppositional tolerance” occurs, in which drugs lose effect.
When the drugs are withdrawn, the over-accommodated nervous system has difficulty finding a homeostasis, generating symptoms that are frequently misdiagnosed as worsening or emergence of a psychiatric disorder.
Either in “oppositional tolerance” or in withdrawal, the nervous system is in a state of compromised integrity and functioning of the body suffers overall. See http://tinyurl.com/7thrxf7
In related news, here is a harrowing patient account of iatrogenic deterioration: http://vitalitymagazine.com/article/an-open-letter-to-doctors/
Every patient who has had a bad experience with psychiatric drugs can relate to this story to some degree. It is archetypal.