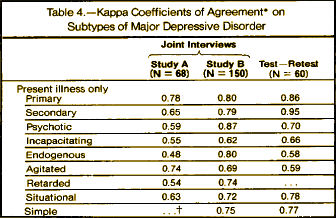
Picking up after the last post, after constructing the Research Diagnostic Criteria, they did an inter-rater reliability study on their subtypes [center column] of Major Depressive Disorder and found fairly respectable Kappa values:
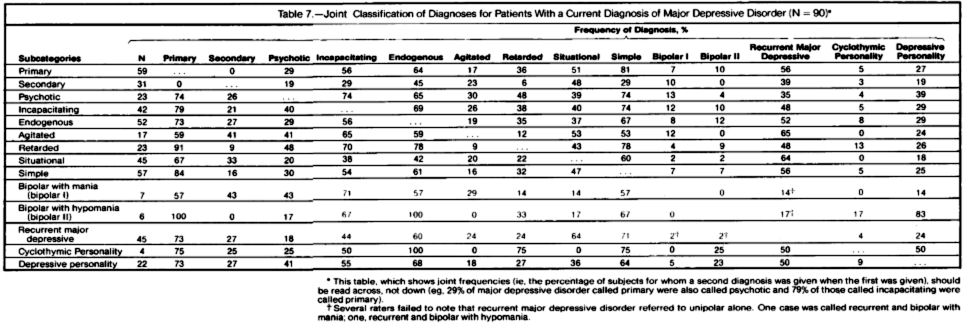
One of the main purposes of the RDC approach to psychiatric diagnosis is to facilitate the comparison of alternative classification systems for depressive disorders. Table 7 gives the joint classification of diagnoses for 90 patients with a current diagnosis of major depressive disorder [study B]. The table should be read across so that the frequency with which subjects given a diagnosis on the left indicates how often they were also given a diagnosis listed on the right. Some of the cell sizes are quite small; therefore, this table is presented primarily for illustrative purposes.Frequently, there is an assumption that the more commonly used methods for classifying depressed patients are equivalent and that the results of studies using these different systems can be easily compared. For example, it is often assumed that episodes of primary depressive disorder would almost always meet the criteria for endogenous depressive disorder and rarely meet the criteria for situational [reactive] depressive disorder. However, only 64% of patients with a diagnosis of primary depressive disorder also met the criteria for endogenous phenomenology, while 51% of them met the criteria for situational depressive disorder. Similarly, it is often assumed that situational (reactive) depressive episodes would rarely meet the criteria for endogenous depressive disorder whereas they actually met those criteria 42% of the time.
It should be noted that the class "neurotic depression," which is one of the most commonly used diagnoses in the standard nomenclature, is not used in the RDC. This term involves too many different meanings to be reliable and valid. Neurotic depression is variously used to mean nonincapacitating, nonpsychotic, nonendogenous, nonrecurring, nonsituational, nonbipolar, due to conflict, or some unspecified combination of all of these features. We believe that each of these features can be better studied separately than by combining them into a single class.
I think that comment about Neurotic Depression was also a mistake. I have no investment in holding on to the category, but the way they dealt with removing it amplified the original mistake to everyone’s detriment. It expressed the opinion of the St. Louis Group and maybe others – a discounting attitude not just towards the psychoanalysts and psychotherapists in psychiatry, but towards a large group of mentally ill patients. It evaporated the diagnoses of the largest cohort of depressed patients, maybe the largest cohort of psychiatric patients, with neither study nor viable alternative. Those patients certainly had no real home in the Research Diagnostic Criteria so the only alternative was to be redistributed among either Major Depressive Disorder or Minor Depressive Disorder [or its later renamings]. The subcategories of Major Depressive Disorder had been developed to parse primarily the Melancholic Depressions, so it was an awkward and unstudied fit [that may explain some of the overlap]. Minor Depressive Disorder was defined as not quite Melancholia or something like that – reinforcing the deconstruction of the categorical distinction. People with the former diagnosis of Neurotic Depression were refugees in a war they didn’t even know was being fought and were scattered among diagnoses that didn’t fit. Changing things to a descriptive base was fine, but making the change without studying the parameters that define this group [or groups] was not only cynical, but grossly unscientific, supposedly in the service of science. And we all know where it ultimately lead.
Minor Depressive Disorder or its heirs like Cyclothymia or Dysthymia never caught on. No matter how they phrased it, it was just a less than diagnosis. The nuances of Melancholia disappeared into the cracks of the latter digits as add-ons and never achieved widespread usage. And so, when it was all said and done, the criteria of a St. Louis psychiatry resident, the Feighner Criteria, was untouched by the RDC or DSM-III processes, trumped the traditional wisdom of psychiatry, and became a unitary diagnosis for any case of significant depression – Major Depressive Disorder. The neuroscientists lost the promising target of Melancholia. There was no legitimate diagnosis for people whose depression arose as a consequence of their life on the planet. And the Pharmaceutical Companies had a category to bet the house on because of its newly inflated size.
It’s not like this problem wasn’t anticipated at the time, apparent in these two snippets from a letter written in 1979 by Dr. Bernard Carroll to Robert Spitzer – an 11th hour plea:
[click the image for the full letter]
Dr. Carroll was prescient.
About 84% of the 31 million Americans over the age of 12 currently on antidepressants have non-endogenomorphic depression (plus some with miscellaneous other conditions, such as IBS, for which antidepressants have been oversold).
The other 16% (about 5 million) are considered to have “severe depressive symptoms,” whatever that means to the CDC (http://www.cdc.gov/nchs/data/databriefs/db76.htm).
Thanks for the compliment, Alto, but actually I don’t think I was prescient. At the time it felt more like I was one of the few persons who wasn’t sleepwalking over the cliff that was MDD. There was nothing prescient to me about my point of view… it was pretty standard non-US stuff that would have been endorsed with minor variations in Europe, the UK, and all the former British colonies like my native Australia. USA was the odd man out when they ran cross-national reliability studies in the late 1960s and early 1970s. Then, the USA ‘solution’ that Mickey has chronicled so well was aimed more at treating US anxieties and issues than at respecting clinical facts about melancholia.
Dr Carroll modestly disclaims prescience; yet his pungent criticism was right on the mark, and we know from the APA Archives that Spitzer felt so stung by it that, after receiving the Carroll letter, he added the “melancholic” subtype to major depression. Would that a single powerful letter might make such a difference with today’s drafters of DSM-V.