In the days before the DSM-III, Manic Depressive Illness began in adulthood with episodes of either Mania or Depression that were self-limited, but tended to be recurrent. The disorder ran in families and we mostly thought of it as a biological "disease." We treated the Manic episodes with Lithium and maybe short-term neuroleptics and the Depressive episodes with Tricyclic Antidepressants or ECT. People had different ideas about long term maintenance and prevention [which made for a good Grand Rounds presentation every year or so]. It was a value-added variant of Emil Kraepelin’s original descriptions. The people in St. Louis thought the rest of us under-diagnosed the condition and over-diagnosed Schizophrenia. The rest of us sort of agreed and the cases diagnosed as "Schizophrenia" that responded to Lithium caught our attention [another recurrent topic for Grand Rounds]. But things were tidier in those days.
Children and adolescents aged 7 to 17 years 11 months (mean±SD age, 13.0±3.1 years) whose primary diagnoses were DSM-IV BP-I or BP-II or an operationalized definition of BP-NOS were enrolled in the COBY study. Because the DSM-IV definition of BP-NOS is vague, BP-NOS was defined as the presence of clinically relevant BP symptoms that did not fulfill the DSM-IV criteria for BP-I or BP-II. In addition, subjects were required to have a minimum of elated mood plus 2 associated DSM-IV symptoms or irritable mood plus 3 DSM-IV associated symptoms, along with a change in the level of functioning, duration of a minimum of 4 hours within a 24-hour period, and at least 4 cumulative lifetime days meeting the criteria.
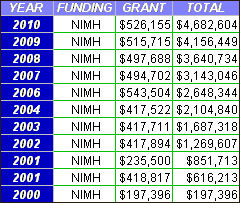 COBY [Course and Outcome of Bipolar Youth] is an ongoing study of Childhood Bipolar Disorder funded by the NIMH [since 2000]. After the initial five year grant [2000-2005] ran out, they got an extension to continue to follow their subjects. They are now following a cohort of 430 children and adolescents to study the course of the disorder into adulthood – something I think is a good idea. As you can see, the Principle Investigator is Dr. Martin Keller of Brown University who became infamous with Study 329, a ghost-written and fallacy laden study of Paxil in the treatment of adolescent depression. COBY is, however, an NIMH funded Study, so it’s worth a look [with reservations]. Here‘s the description from that extension request:
COBY [Course and Outcome of Bipolar Youth] is an ongoing study of Childhood Bipolar Disorder funded by the NIMH [since 2000]. After the initial five year grant [2000-2005] ran out, they got an extension to continue to follow their subjects. They are now following a cohort of 430 children and adolescents to study the course of the disorder into adulthood – something I think is a good idea. As you can see, the Principle Investigator is Dr. Martin Keller of Brown University who became infamous with Study 329, a ghost-written and fallacy laden study of Paxil in the treatment of adolescent depression. COBY is, however, an NIMH funded Study, so it’s worth a look [with reservations]. Here‘s the description from that extension request:
| Project Number: | 2R01MH059691-06A2 | Contact Principal Investigator: | KELLER, MARTIN B |
| Title: | COURSE AND OUTCOME FOR BIPOLAR DISORDER IN YOUTH (COBY) | Awardee Organization: | BROWN UNIVERSITY |
|
|
|||
|
DESCRIPTION (provided by applicant): This competing continuation of the study "Course and Outcome of Bipolar Youth" (COBY) will extend the follow-up of the sample for 5 more years. COBY is collaboration by the University of Pittsburgh, Brown University, and UCLA to investigate the longitudinal course of pediatric bipolar disorder (BP). As of 10/1/2005, we achieved our recruitment goal of 430 youth (186 children and 244 adolescents) with BP spectrum disorders (I, II and Not Otherwise Specified–NOS) using state-of-the-art clinical and analytic methodologies. Preliminary analyses of COBY’s data are showing that pediatric BP is a rapid fluctuating and chronic illness associated with high psychosocial morbidity. However, limited data exists on the phenomenology, treatment responsiveness, and how course is influenced by the developmental transitions from childhood to adolescence, and adulthood. The unprecedented scientific and public health implications of COBY will accrue from ongoing observational data on a large, clinically diverse cohort of rigorously diagnosed subjects, which will enable us to: (1) describe the naturalistic course of recovery and recurrence patterns, as well as rapid mood changes, subsyndromal symptoms, and well periods into early adulthood; (2) identify predictors of long-term course and outcome; (3) describe psychosocial outcomes from childhood to early young adulthood; (4) describe treatments received and their effects in mediating course patterns; and 5) to explore domains of cognitive functioning across development in children and adolescents with BP spectrum disorders. Beyond the acquisition of new knowledge about long-term temporal patterns of pediatric-onset BP, an intrinsic value of extending the study of our cohort for another 5 years is that we will determine whether, and how, clinical phenotypes, psychopathological course trajectories, cognitive development and other important outcome variables change as probands move across developmental stages from childhood to young adulthood. Continued follow-up of the COBY sample at 6-month intervals using adaptations of instruments from the successful adult Collaborative Depression Study (CDS), will make it possible to develop more comprehensive knowledge on the above-noted aims given its large size, ascertainment from multiple sites, demographic and clinical diversity, and inclusion of subjects across the broad range of disease severity.
|
|||
So here’s the initial report of their results in 2006 [the link is the full text]:
Clinical course of children and adolescents with bipolar spectrum disorders.
by Birmaher B, Axelson D, Strober M, Gill MK, Valeri S, Chiappetta L, Ryan N, Leonard H, Hunt J, Iyengar S, and Keller M.
Archives of General Psychiatry. 2006 63(2):175-83.
AbstractDespite the high morbidity associated with bipolar disorder (BP), few studies have prospectively studied the course of this illness in youthOBJECTIVE: To assess the longitudinal course of BP spectrum disorders (BP-I, BP-II, and not otherwise specified [BP-NOS]) in children and adolescents.DESIGN: Subjects were interviewed, on average, every 9 months for an average of 2 years using the Longitudinal Interval Follow-up Evaluation.SETTING: Outpatient and inpatient units at 3 university centers.PARTICIPANTS: Two hundred sixty-three children and adolescents (mean age, 13 years) with BP-I (n = 152), BP-II (n = 19), and BP-NOS (n = 92).MAIN OUTCOME MEASURES: Rates of recovery and recurrence, weeks with syndromal or subsyndromal mood symptoms, changes in symptoms and polarity, and predictors of outcome.RESULTS: Approximately 70% of subjects with BP recovered from their index episode, and 50% had at least 1 syndromal recurrence, particularly depressive episodes. Analyses of weekly mood symptoms showed that 60% of the follow-up time, subjects had syndromal or subsyndromal symptoms with numerous changes in symptoms and shifts of polarity, and 3% of the time, psychosis. Twenty percent of BP-II subjects converted to BP-I, and 25% of BP-NOS subjects converted to BP-I or BP-II. Early-onset BP, BP-NOS, long duration of mood symptoms, low socioeconomic status, and psychosis were associated with poorer outcomes and rapid mood changes. Secondary analyses comparing BP-I youths with BP-I adults showed that youths significantly more time symptomatic and had more mixed/cycling episodes, mood symptom changes, and polarity switches.CONCLUSIONS: Youths with BP spectrum disorders showed a continuum of BP symptom severity from subsyndromal to full syndromal with frequent mood fluctuations. Results of this study provide preliminary validation for BP-NOS.
[reformatted to fit your screen 1bom]
…the observed outcomes were in the context of naturalistically applied treatment.andAs has been reported by others, subjects in whom BP symptoms developed during their early childhood showed lower rates of recovery, more time in mixed/ rapid cycling episodes, and more symptom and polarity changes than those whose illness started later. Also, comparable with recent adult BP studies,53,56 the results of the COBY study consistently showed that BP subjects with low SES had worse prognosis. Future studies will evaluate possible factors (eg, exposure to negative life events, lack of or poor adherence to treatment, and increased family psychopathologic characteristics) that may account for this finding.
Four-Year Longitudinal Course of Children and Adolescents With Bipolar Spectrum Disorders: The Course and Outcome of Bipolar Youth [COBY] Study
by Boris Birmaher, David Axelson, Benjamin Goldstein, Michael Strober, Mary Kay Gill, Jeffrey Hunt, Patricia Houck, Wonho Ha, Satish Iyengar, Eunice Kim, Shirley Yen, Heather Hower, Christianne Esposito-Smythers, Tina Goldstein, Neal Ryan, and Martin Keller
American Journal of Psychiatry 2009 166:795-804.
AbstractThe authors sought to assess the longitudinal course of youths with bipolar spectrum disorders over a 4-year period.METHOD: At total of 413 youths (ages 7-17 years) with bipolar I disorder (N=244), bipolar II disorder (N=28), and bipolar disorder not otherwise specified (N=141) were enrolled in the study. Symptoms were ascertained retrospectively on average every 9.4 months for 4 years using the Longitudinal Interval Follow-Up Evaluation. Rates and time to recovery and recurrence and week-by-week symptomatic status were analyzed.RESULTS: Approximately 2.5 years after onset of their index episode, 81.5% of the participants had fully recovered, but 1.5 years later 62.5% had a syndromal recurrence, particularly depression. One-third of the participants had one syndromal recurrence, and 30% had two or more. The polarity of the index episode predicted that of subsequent episodes. Participants were symptomatic during 60% of the follow-up period, particularly with subsyndromal symptoms of depression and mixed polarity, with numerous changes in mood polarity. Manic symptomatology, especially syndromal, was less frequent, and bipolar II was mainly manifested by depressive symptoms. Overall, 40% of the participants had syndromal or subsyndromal symptoms during 75% of the follow-up period, and 16% of the participants experienced psychotic symptoms during 17% the follow-up period. Twenty-five percent of youths with bipolar II converted to bipolar I, and 38% of those with bipolar disorder not otherwise specified converted to bipolar I or II. Early onset, diagnosis of bipolar disorder not otherwise specified, long illness duration, low socioeconomic status, and family history of mood disorders were associated with poorer outcomes.CONCLUSIONS: Bipolar spectrum disorders in youths are characterized by episodic illness with subsyndromal and, less frequently, syndromal episodes with mainly depressive and mixed symptoms and rapid mood changes.
[reformatted to fit your screen 1bom]
In summary, although distinct episodes of full syndromal mood symptomatology as well as durable periods of euthymia can be identified in youths with bipolar disorder, the course of bipolar spectrum disorders in children and adolescents is predominantly characterized by subsyndromal and, much less frequently, syndromal episodes. Rapid mood changes are evident during these episodes, which are mainly of depressive and mixed polarity. During follow-up each bipolar subtype showed some distinct clinical characteristics and course, but there was overlap in their symptoms and substantial conversion from bipolar II and bipolar disorder not otherwise specified into other bipolar subtypes. The course of bipolar disorder, the relative infrequency of syndromal DSM manic episodes, the effects of development in symptom manifestation, and the high prevalence of comorbid disorders may account, at least in part, for the difficulties in recognizing and managing this illness in youths. The recurrence, chronicity, and psychosocial morbidity associated with this illness in critical developmental stages call for its prompt recognition and the development of more efficacious treatments, particularly since each year of illness appears to decrease the likelihood of recovery.
“In the days before the DSM-III, Manic Depressive Illness began in adulthood with episodes of either Mania or Depression that were self-limited, but tended to be recurrent.”
That conflicts with the long-term observations of Kraepelin — before the advent of medications, DSM-whatever, or any KOLs. — that manic-depression begins in youth.
Now, I see that you mentioned Kraepelin, with the “value-added” comment. In my opinion, Kraepelin would not agree that the views expressed above are in any way based (to be “value-added”) on his views.
The “value” I’m talking about as “added” is effective treatment. And as my next post says, I agree with you that they have a respectable number of kids cases. I just think it’s overdone [because it is]…
Thanks for your response. While I respect your views, I don’t agree with all of them. On the idea of kids’ cases being overdone …
From my reading of the subject, most bipolar and schizophrenia would be “kids’ cases” since, as Kraepelin observed, the illnesses start in youth. And since youth today, especially girls, go through puberty earlier than in Kraepelin’s day …
Anyway, I’ll no doubt be responding to the next post! In the meantime, have a great 4th of July weekend.
[…] In a couple of earlier posts, I admitted to the existence of Childhood Bipolar Disorder [bipolar kids: COBY [Course and Outcome of Bipolar Youth…, bipolar kids: my take from COBY…]. But I totally agree with Dr. Frances that the […]