In a psychotherapy, one hears people say some mighty peculiar things, things that make no sense at all. It’s fairly easy to see how the belief underlying those odd things might be causing the difficulty that brought them to treatment in the first place. But just identifying a maladaptive belief and its connection to their symptoms is only start. The first order of business is to find out what the thing that made no sense means to them. In my last post, I said that Dr. John Krystal’s comment "Instead she attacks the one clear path to better diagnoses and more effective pharmacotherapies, translational neuroscience." made absolutely no sense to me [poltergeists make up the principal type of spontaneous material manifestation…]. But I’m not Dr. John Krystal, nor am I the President of the American College of Neuropsychopharmacology. So, in this case, I’d better reconsider my own understanding of what transitional neuroscience actually means. I took it to mean accelerating basic scientific discovery through the process it takes to make it clinically useful – "bench to bedside" as they say. That’s not at all what Dr. Krystal means. And the path to his meaning is pretty easy to follow. Just go to the National Center for Advancing Translational Sciences [NCATS] website.
On July 24, 2012, NIH issued 17 awards for research projects designed to create 3-D chips with living cells and tissues that accurately model the structure and function of human organs, such as the lung, liver and heart. Ten of these awards will support studies to develop 3-D cellular microsystems that represent a number of human organ systems. These bio-engineered devices will be functionally relevant and accurately reflect the complexity of the tissue of origin, including genomic diversity, disease complexity and pharmacological response. Seven awards will explore the potential of stem and progenitor cells to differentiate into multiple cell types that represent the cellular architecture within organ systems. These could act as a source of cells to populate tissue chips.
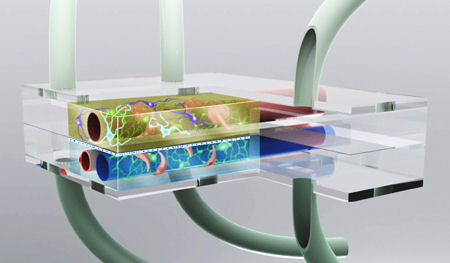
Artist’s conception of the microbrain bioreactor. The upper chamber contains the neurons and an artificial capillary that carries blood to the brain surrounded by the cells that make up the blood-brain barrier. The lower layer is filled with cerebral spinal fluid and contains an artificial choroid plexus that makes CSF and a venule that carries blood away from the brain, along with a collection of cells that form the blood-CSF and CSF-brain barriers. Collectively, all these cells will reproduce the microenvironment found in the brain. The entire device will be about the size of a grain of rice.
|
 Welcome to the National Center for Advancing Translational Sciences at the NIH. Our mission is to catalyze the generation of innovative methods and technologies that enhance the development, testing, and implementation of diagnostics and therapeutics across a wide range of human diseases and conditions. Advances in these areas will enable others in both the public and private sectors to develop drugs and diagnostics more efficiently for any number of human diseases — ultimately accelerating the pace in which new therapeutics are delivered to the patients who need them. In establishing the Center, NIH involved internal and external stakeholders to guide its research agenda and pinpoint priorities. A group of NIH Institute and Center directors, including those most involved in translational research, emphasized the need for a translational focus that would provide tools and resources to facilitate research across NIH. Additionally, a working group of the NIH Advisory Committee to the Director, comprised of experts from industry, private equity firms, nonprofit organizations and academia, identified a need to streamline translational sciences. Priority areas included: Welcome to the National Center for Advancing Translational Sciences at the NIH. Our mission is to catalyze the generation of innovative methods and technologies that enhance the development, testing, and implementation of diagnostics and therapeutics across a wide range of human diseases and conditions. Advances in these areas will enable others in both the public and private sectors to develop drugs and diagnostics more efficiently for any number of human diseases — ultimately accelerating the pace in which new therapeutics are delivered to the patients who need them. In establishing the Center, NIH involved internal and external stakeholders to guide its research agenda and pinpoint priorities. A group of NIH Institute and Center directors, including those most involved in translational research, emphasized the need for a translational focus that would provide tools and resources to facilitate research across NIH. Additionally, a working group of the NIH Advisory Committee to the Director, comprised of experts from industry, private equity firms, nonprofit organizations and academia, identified a need to streamline translational sciences. Priority areas included:
Through this guidance, NCATS is ensuring that its research efforts are not duplicating the efforts of others at NIH or competing with industry. As such, our highest priority is to reduce, remove or bypass significant hurdles across the continuum of translational research, particularly in the priority areas indicated above by our stakeholders. As a result, the NCATS research agenda reflects this goal, and our current budget request is aligned with these priorities. All of us at NCATS are excited about the opportunities on the horizon to advance translational sciences. As you explore our new website, check back often to learn about the Center’s latest news, like us on Facebook and join our Twitter feed. As always, we welcome your feedback on ways to improve the site. Thomas R. Insel, M.D.
Acting Director National Center for Advancing Translational Sciences |
Looked at that site yesterday. $ was on the face of it, down to the link to the Forbes article. I’m all for happy government supported research efforts, but cellular psychology?
psychiatry
I say it’s spinach, and I say the hell with it.
Not to be long-winded, but…. A few weeks ago, I wrote an e-mail to Dr. Insel about his blog post on “Experimental Medicine”, asking if the inability so far to find good medications might suggest that mental disorders on the whole are simply not very amenable to medication-based solutions. I was curious about NIH pursuing further non-medication research, and suggested that additional qualitative studies — actually asking the patients themselves more about their first-hand experiences and perspectives on healing — might lead to additional hypotheses that can then be tested using quantitative studies.
To his credit, Dr. Insel replied to me within a few days. I don’t want to mis-paraphrase his reply. He didn’t address my suggestion about qualitative research, but he invoked nonverbal children with autism and adults with severe schizophrenia as examples of people most in need better treatments, and asking why forsake this important component of treatment (medication) for those with the most disabling illnesses in medicine. (I’ve seen before that “advocates” like this will often invoke the “most seriously ill”, principally those who are less able to clearly express themselves, in order to push the advocates’ own agenda.)
I wrote back (this time including a bunch of citations), suggesting that there’s actually good news for people with those two conditions. There’s increasing discovery that “nonverbal” people with autism doesn’t necessarily imply noncommunicative, but that some can make use of augmentive communication tools and methods with varying degrees of success. And the increasing awareness that many people diagnosed with schizophrenia go on to recover, to a much greater degree than was previously believed possible (often without medications), opens additional exciting areas for research to pursue. I also wondered aloud if a more “rehabilitative” approach (working closely and cooperatively with the people in distress) might be helpful. I reiterated my increasing doubt whether serious mental illnesses necessarily involve molecular targets responsive to medications, and my curiosity about qualitative research as a way of learning more about what people have personally found helpful in their own healing journeys.
Dr. Insel understandably didn’t reply to my followup, but I didn’t expect that he would want to have an ongoing exchange with some Phil Q. Public guy who e-mailed him. I’m a bit of a science geek, and in my view, some of these “contrary” findings about mainstream psychiatry actually suggest some exciting new areas of research (e.g. learning more about what actually helps people the most), and I’m ticked off that the researchers don’t seem to look at it that way.
Well, I do declare! I could not have imagined a higher level of dehumanizing –the human being for [fun?] and profit! Of course this is what we want our tax dollars funding–research and development of robotic/computerized models for testing more toxic-waste-of-time-drugs… that will reduce our lifespan or kill us outright.
Wonder if the latest mass murdering psychiatric patient was studying *Translational Neuroscience* — Holmes was studying on the taxpayers dime. Perhaps he was being groomed for this *project*???
This pie-in-the-sky is Krystal (and Insel) yearning for psychiatry to be among the real sciences.
Chip technology has been kicking around biotech for 20 years. “Organs on a chip” concepts are a dime a dozen. See http://www.genengnews.com/gen-news-highlights/creating-a-human-body-on-a-chip/81247095/
Psychiatry’s problem will be applicability. What does a result that takes place in a soup of [emulated] amino acids mean in real humans?
Altostrata…. there isn’t much evidence that psychiatrists believe they have been treating REAL humans! 😉