Newsflash From APA Meeting: DSM 5 Has Flunked its Reliability Tests
Needs To Be Kept Back For Another Year
DSM5 in Distress: Psychology Today
by Allen J. Frances, M.D.
May 6, 2012
The whole purpose of having a manual of psychiatric diagnosis is to promote diagnostic agreement. DSM III was an important milestone because it saved the credibility and relevance of psychiatry at a time when it was ridiculed for low reliability. Everyone knew that the reliability achieved in DSM field testing far exceeds what is possible in clinical practice, but DSM III took the major step of proving that reliability could be achieved at all. Until now, the DSM’s have facilitated communication across the clinical/research interface, promoted research, and provide credibility in the court room.But bad news has just been reported from the annual meeting of the American Psychiatric Association in Philadelphia. The hard won credibility of psychiatric diagnosis is compromised by the abysmal results reported by the DSM 5 Field Trials. This failure was clearly predictable from the start:
[1] The writing of the DSM 5 criteria sets was far too raw and imprecise to be ready for the rigors of field testing. The ambiguity cried out for expert editing; without which reasonable reliability is impossible;
[2] The design of the field trial was byzantine in complexity and could never be done on schedule:
[3] Constant delays in starting and completing Stage 1 of the study forced DSM 5 to cancel the planned Stage 2 that was meant to clean up the poorly performing criteria sets identified in the first stage.
[4] With stage 2 cancelled without explanation, it looks like even the worst diagnoses are being given a social pass; and, most absurd,
[5] The design was totally off point, failing to ask the only question that really counted [the impact of DSM 5 on rates].
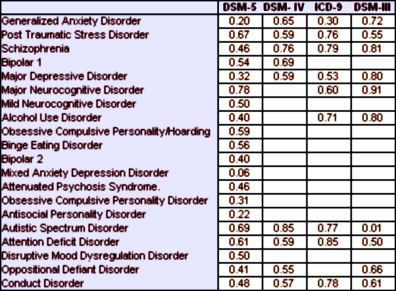
The results of the DSM 5 field trials are a disgrace to the field. For context, in previous DSM’s, a diagnosis had to have a kappa reliability of about 0.6 or above to be considered acceptable. A reliability of 0.2-0.4 has always been considered completely unacceptable, not much above chance agreement:Kappa Values from the DSM-5 Field Trials
[reformatted from the original]No predetermined publication date justifies business as usual in the face of these terrible Field Trial results [which are even more striking since they were obtained in academic settings with trained and skilled interviewers, highly selected patients, and no time pressure. The results in real world settings would be much lower]. Reliability this low for so many diagnoses gravely undermines the credibility of DSM 5 as a basis for administrative coding, treatment selection, and clinical research.What can be done to salvage this deplorable mess:
[1] DSM 5 has never had anyone on board who could write a clean, consistent, unambiguous criteria set. DSM 5 received either no editing at all or amateur editing. Getting the words right is certain not enough- but If you can’t get them right, nothing else can ever be safe.
[2] For DSM 5 to retrieve credibility, it complete the second planned stage of its field testing. If doing the job right must delay publication so be it. Public trust must trump private publishing profits and it is self defeating for APA to publish a book no one can trust.I have been consistently pessimistic and critical about DSM 5 since my first piece on it 3 years ago. The sad thing is I can still be so surprised. Each step of the way I predict it will fail in one or another way. But then I discover that DSM 5 has managed to fail in ways that go beyond my poor imagination. This assault on reliability was predicted, but its scope exceeds even my jaundiced fears and creates a DSM 5 emergency.
If this is what leadership is for my profession, psychiatry is dead for whatever professional efforts were left prior to this meeting. I feel vindicated that my lack of trust and respect for older established colleagues has been validated for the most part. These guys and gals who run the APA and major academic centers are beyond corrupt and inept. I feel it fair to say there is an antisocial element, if not at least a pathetically pathological narcissistic element, that drives these KOLs to to think solely for their wallets, egos, and prestige, and almost solely at the price of patient care.
Again, how does anyone with a soul and conscience belong to the APA as of 2012, hell, to me since 2000? If that question offends, well, now you know how I have felt these past 10 or more years having to endure colleagues telling me to listen and respect the APA and academia for knowing what is best for the profession.
If you are hoping to practice psychiatry for another 15 or 20 years or more, good luck! We will be irrelevant by the next 3 or 4 years at best. And be sure to thank the bastard(s) who coined that wonderful adage “biochemical imbalance”. We literally dug our own graves, handed the shovel to our traitors, and turned our backs to let them strike us in the back of the heads to fall in the pit!
Harsh comment? Try listening to endless debate and demands for meds from patients in any element of mental health care these past few years. I just want to know how therapists expect to survive when I figure at best 20% of people in community mental health responsibly participate in therapy, and lucky if even that in private practice of late. And I am not even talking about benzo and stimulant seeking.
Forgive my ignorance here and probably a stupid question. Is there a relationship between kappa values and chance? For example my flipping a coin and my guessof it being heads has a 50% chance of being correct. If I can continually prove my predictive power is greater than that I presume I have knowledge. Is there anywhere I can read up on Kappa values? I will search on google. Thanks.
Will it really be the end for psychiatry? Surely people will just carry on with DSM- IV until the APA get their house in order.
Great summary of the problem though – thanks.
Nick,
See box scores and kappa…