Posted on Friday 1 May 2015
hat tip to pharmagossip…
Comments Off on net·flix…


Pharmalot: WSJBy Ed Silverman04/29/2015
Otsuka Pharmaceuticals was dealt a setback yesterday when the FDA approved four generic versions of its best-selling Abilify® antipsychotic pill, following an unusual and protracted legal battle. Shortly thereafter, Teva Pharmaceuticals announced that it was launching a copycat medicine. The move comes after Otsuka cited complex regulatory law to thwart generics, but the agency rejected the argument and decided that generic versions meet the standard for approval… And Otsuka also has a great deal at stake – Abilify® generated $4.9 billion in U.S. sales last year.
As we wrote previously, the FDA late last year approved Abilify® for treating children with Tourette syndrome, a neurological disorder that causes tics. Since Abilify® had a so-called orphan designation, which refers to a drug used to treat a rare malady like Tourette’s, Otsuka won another seven years of exclusive marketing rights – through late 2021 – before low-cost generics could appear.
But in February, the FDA surprised Otsuka by approving Abilify® to treat adults with Tourette syndrome. This widened the market, but Otsuka contends FDA law would trigger a labeling change that could usher in generics. Otsuka filed a lawsuit claiming the FDA isn’t allowed to approve an indication for which a drug maker didn’t apply and charged the agency
was actually attempting to usher in generic copies.
For its part, the FDA backpedaled and earlier this month told Otsuka that Abilify® was now approved to treat Tourette syndrome, but only for children. However, the agency also indicated it may use a so-called carve-out approach to approve generics for treating psychiatric disorders, but not Tourette syndrome. And that is what the FDA did Tuesday…
by Correll CU, Skuban A, Ouyang J, Hobart M, Pfister S, McQuade RD, Nyilas M, Carson WH, Sanchez R, and Eriksson H.American Journal of Psychiatry. 2015 Apr 16 [Epub ahead of print]
by Kane JM, Skuban, Ouyang, Hobart, Pfister, McQuade, Nyilas, Carson, Sanchez, and Eriksson.Schizophrenia Research. 2015 Feb 12. [Epub ahead of print]
by W. Wolfgang Fleischhacker, Raymond Sanchez, Pamela P. Perry, Na Jin, Timothy Peters-Strickland, Brian R. Johnson, Ross A. Baker, Anna Eramo, Robert D. McQuade, William H. Carson, David Walling and John M. KaneThe British Journal of Psychiatry. 2014 205:135–144.FundingThis study was supported by Otsuka Pharmaceutical Commercialization, Inc. [Tokyo, Japan]. Editorial support for the preparation of this manuscript was provided by Suzanne Patel at Ogilvy Healthworld Medical Education and Amy Roth Shaberman, PhD, and Brett D. Mahon, PhD, at C4 MedSolutions, LLC, a CHC Group company; funding was provided by Otsuka Pharmaceutical Commercialization, Inc. and H. Lundbeck A/S.AcknowledgementsThe authors would like to thank Svetlana Ivanova, PhD, Otsuka Pharmaceutical Development & Commercialization, Inc., Rockville, MD, USA, for her contribution to the analysis and interpretation of data.
So we wonder who is on the faculty of this Free CME? I clicked on the link to Adherence, Recovery, and the Role of LAIs in Schizophrenia:Faculty
Professor of Psychiatry and Molecular Medicine
Hofstra North Shore – LIJ School of MedicineMedical Director of Recognition and Prevention (RAP) Program
The Zucker Hillside Hospital
Glen Oaks, NY
Professor of Psychiatry
Hofstra North Shore – LIJ Health System School of Medicine
Vice President
Behavioral Health Services of the North Shore – LIJ Health System
Chairman of Department of Psychiatry and Chief of Staff
The Zucker Hillside Hospital
Glen Oaks, New York
Chancellor’s Chair of Excellence in Psychiatry
Executive Medical Director of the Missouri Psychiatric Center
School of Medicine, University of Missouri Health System
Columbia, MOTake a look at the Learning Objective and guess what you’re going to learn – for free. Oh by the way, John Lauriello, MD is the senior author of a glowing handout review of Abilify®Maintena.
In the spice must flow…, I joked "[it was one·stop shopping for both ghost·writers and KOLs]," but it was bigger than I knew. The Hofstra faculty provided not only authors for both Brexpiprazole papers, but also the Abilify®Maintena paper and the Abilify®Maintena CME – all of which were aimed at holding onto the market as Abilify® becomes generic. This was one·stop shopping-maximus [though Abilify®Maintena did get different ghost-writers]. The Abilify®Maintena study had 98 sites!
 Guest Authors: In this case, the articles are no longer crammed with academics like a decade ago. I guess it only takes one to be the ticket into an academic journal. In this case, the main authors came from Hostra [The Feinstein Institute] for the articles and C.M.E. Their C.V.s and C.O.I. are heavily weighted with Clinical Trials of drugs.
Guest Authors: In this case, the articles are no longer crammed with academics like a decade ago. I guess it only takes one to be the ticket into an academic journal. In this case, the main authors came from Hostra [The Feinstein Institute] for the articles and C.M.E. Their C.V.s and C.O.I. are heavily weighted with Clinical Trials of drugs.
 Well, this can’t be a book review of Lieberman’s and Ogasi’s Shrinks, the Untold Story of Psychiatry or Whitaker’s and Cosgrove’s Psychiatry under the Influence because I’ve read neither, but we all have a pretty good take on what they’re about. What struck me is that the titles could be interchanged, and they would still work. Lieberman’s book continues the well worn theme that the 1980 revolution ushered in by the DSM-III in which Psychiatry was liberated from Psychoanalysis and put on the path of true science – so he could’ve worked with a title like Psychiatry under the Influence. And Whitaker and Cosgrove could’ve gone with Shrinks, The Untold Story of Psychiatry to illustrate how much the post-1980 version of Psychiatry has been
Well, this can’t be a book review of Lieberman’s and Ogasi’s Shrinks, the Untold Story of Psychiatry or Whitaker’s and Cosgrove’s Psychiatry under the Influence because I’ve read neither, but we all have a pretty good take on what they’re about. What struck me is that the titles could be interchanged, and they would still work. Lieberman’s book continues the well worn theme that the 1980 revolution ushered in by the DSM-III in which Psychiatry was liberated from Psychoanalysis and put on the path of true science – so he could’ve worked with a title like Psychiatry under the Influence. And Whitaker and Cosgrove could’ve gone with Shrinks, The Untold Story of Psychiatry to illustrate how much the post-1980 version of Psychiatry has been Lieberman: “Is [Whitaker] wrong? What he says is preposterous. He’s a menace to society because he’s basically fomenting misinformation and misunderstanding about mental illness and the nature of treatment. What he just said in that clip you ran about, if you’re taking an antidepressant and you go off it and you get sick again… the same thing could be said about insulin for diabetes and asthma medication… Whitaker, he ostensibly considers himself to have been a journalist, God help the publication that employed him, but he has an ideological grudge against psychiatry for whatever reason and there’s no, what he calls research is simply his opinion and his construction of information."Enright: "What about his contention that the unmedicated patients did better than the medicated patients?"Lieberman: "I’d say that’s absolutely wrong. If you do a controlled study with various illnesses, whether it’s schizophrenia, depression, bipolar disorder, obsessive compulsive disorder, and you do a randomized study, assign one group to receive whatever the state of the art is in psychiatry including medication and you assign the other to some innocuous, non-medical type of supportive therapy or whatever, and you follow the people for a period of time the outcomes will be extraordinarily superior in the treated group. The magnitude of the difference we can sort of quibble about, but there’s no doubt about it."
So here is our challenge to Dr. Lieberman. Please provide a list of randomized studies that show that medicated patients have a much better long-term outcome than the unmedicated patients. Please note that we are asking for studies that measure outcomes over the long-term, say for at least two years or longer, and are randomized, since you indicate there are many such studies. Please point out the “extraordinarily superior” outcomes for the medicated group. We presume the studies will focus not just on symptom control, but also functional outcomes…
This is not the first time Lieberman has denounced me as a crappy journalist. [See CV here.] After Mad in America was published, we were on a National Public Radio show together, where he said that my book was a travesty that set journalism back decades [as apparently I had failed to get in line with the rest of journalists writing about the wonders of modern psychiatry]. He has written other things very similar to what he told Michael Enright on Sunday, but I have to confess, I took extra pride in being called a “menace to society.” I think one day I will put that on my gravestone.
Dr. Lieberman obviously sees himself as the champion and spokesman for Psychiatry. It seems to antedate his tenure as APA President. In September 2011, not long after the DSM-5 Task Force had to abandon the attempt to create a "biological" classification and it became apparent that PHARMA was closing its CNS Drug research labs, Lieberman recorded a MedScape video [Psychiatric Diagnosis in the Lab: How Far Off Are We?] about the neuroscience breakthroughs that were just around the corner. He has continued to be a cheerleader for APA and his own brand of Psychiatry [DSM-5: Caught between Mental Illness Stigma and Anti-Psychiatry Prejudice, Our Time Has Come, Psychiatry Hits its Stride as Brain Science Informs Treatment], and has continued to push for a strong relationship with PHARMA [Don’t Turn Your Back on Industry, but Keep It Honest, APF Convenes Unique Pipeline Summit, Time to Re-Engage With Pharma?]. One could make the case that he is the leading [or at least the loudest] voice for the Guild of Psychiatry.
The article about mental illness was an incredibly unscholarly, misinformed, confused — at worst, unhelpful, and at best, destructive — commentary that will add to the confusion about the diagnosis of mental illness, enhance the stigma, and may lead some patients to doubt the veracity of the diagnoses that they have been given and the treatments that they are receiving…Finally, when I read the article, disappointed and annoyed as I was, I tried to write a serious, responsible, and constructive letter to the editor, which I submitted within 24 hours. Seventy-two hours have elapsed since the article’s publication. I haven’t heard from the Times about their interest in publishing my response, so I assume they won’t publish it. The name that I publish under is my own. My credential is the Chairman of Psychiatry, Columbia University College of Physicians and Surgeons, one of the leading departments of psychiatry in the country, past president of the American Psychiatric Association, and author of the forthcoming book for the lay public called Shrinks: The Untold Story of Psychiatry.
Assuming that my letter was not completely uninformed or incoherent, I would think that there would have been reason to accept it, given my credentials and the fact that I made a reasonable point. Let’s see if they print it. If they don’t, that adds further to my dismay over what I consider to be journalistically irresponsible behavior by this once-respected newspaper.
by Matthew P. Hyett, Michael J. Breakspear, Karl J. Friston, Christine C. Guo, and Gordon B. ParkerJAMA Psychiatry. 2015 72[4]:350-358.
IMPORTANCE Patients with melancholia report a distinct and intrusive dysphoric state during internally generated thought. Melancholia has long been considered to have a strong biological component, but evidence for its specific neurobiological origins is limited. The distinct neurocognitive, psychomotor, and mood disturbances observed in melancholia do, however, suggest aberrant coordination of frontal-subcortical circuitry, which may best be captured through analysis of complex brain networks.OBJECTIVE To investigate the effective connectivity between spontaneous [resting-state] brain networks in melancholia, focusing on networks underlying attention and interoception.DESIGN, SETTING, AND PARTICIPANTS We performed a cross-sectional, observational, resting-state functional magnetic resonance imaging study of 16 participants with melancholia, 16 with nonmelancholic depression, and 16 individuals serving as controls at a hospital-based research institute between August 30, 2010, and June 27, 2012.We identified 5 canonical resting-state networks [default mode, executive control, left and right frontoparietal attention, and bilateral anterior insula] and inferred spontaneous interactions among these networks using dynamic causal modeling.MAIN OUTCOMES AND MEASURES Graph theoretic measures of brain connectivity, namely, in-degree and out-degree of each network and edge connectivity, between regions composed our principal between-group contrasts.RESULTS Melancholia was characterized by a pervasive disconnection involving anterior insula and attentional networks compared with participants in the control [Mann-Whitney, 189.00; z = 2.38; P = .02] and nonmelancholic depressive [Mann-Whitney, 203.00; z = 2.93; P = .004] groups. Decreased effective connectivity between the right frontoparietal and insula networks was present in participants with melancholic depression compared with those with nonmelancholic depression [χ² = 8.13; P = .004]. Reduced effective connectivity between the insula and executive networks was found in individuals with melancholia compared with healthy controls [χ² = 8.96; P = .003].CONCLUSIONS AND RELEVANCE We observed reduced effective connectivity in resting-state functional magnetic resonance imaging between key networks involved in attention and interoception in melancholia. We propose that these abnormalities underlie the impoverished variety and affective quality of internally generated thought in this disorder.
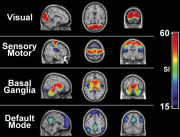 [This is a rough stab at introducing their methodology from one boring old psychoanalyst – so be gentle]. 25 years ago, Seiji Ogawa discovered that the MRI could detect the difference between oxygenated and deoxegenated hemoglobin. Since neuronal activity uses oxygen, it meant that we could actually see areas of increased neuronal activity in the brain – the blood-oxygen-level dependent contrast imaging or BOLD technique. We’ve all seen the pictures of areas in the brain lighting up in response to various stimulus. Attention then turned to the brain at rest, without stimuli [Resting state fMRI] where a number of consistent functional areas have been identified. These functional areas in the resting fMRI are connected, detected by timeline studies of simultaneous activity, so connection [and the direction of these connections] can be determined by some statistical/mathematical analyses beyond comprehension by most of the earth’s population – certainly mine. These connections [networks] may be visible [eg connectomes] or functional. Thus ends my stab at an intro to their methodology.
[This is a rough stab at introducing their methodology from one boring old psychoanalyst – so be gentle]. 25 years ago, Seiji Ogawa discovered that the MRI could detect the difference between oxygenated and deoxegenated hemoglobin. Since neuronal activity uses oxygen, it meant that we could actually see areas of increased neuronal activity in the brain – the blood-oxygen-level dependent contrast imaging or BOLD technique. We’ve all seen the pictures of areas in the brain lighting up in response to various stimulus. Attention then turned to the brain at rest, without stimuli [Resting state fMRI] where a number of consistent functional areas have been identified. These functional areas in the resting fMRI are connected, detected by timeline studies of simultaneous activity, so connection [and the direction of these connections] can be determined by some statistical/mathematical analyses beyond comprehension by most of the earth’s population – certainly mine. These connections [networks] may be visible [eg connectomes] or functional. Thus ends my stab at an intro to their methodology.  What Matthew Hyett et al did was to run resting fMRIs on 16 subjects each, from three cohorts – normals, non-melancholic depressed people, and a group with Melancholia. They identified five of the functional areas and studied their connectivity in each group. What they found was a clear separation among the three groups – documenting "reduced effective connectivity in resting-state functional magnetic resonance imaging between key networks involved in attention and interoception in melancholia."
What Matthew Hyett et al did was to run resting fMRIs on 16 subjects each, from three cohorts – normals, non-melancholic depressed people, and a group with Melancholia. They identified five of the functional areas and studied their connectivity in each group. What they found was a clear separation among the three groups – documenting "reduced effective connectivity in resting-state functional magnetic resonance imaging between key networks involved in attention and interoception in melancholia."
Despite advances in pursuing the neurobiological causes of clinical depressive conditions, the literature is characterized by divergent findings, likely reflecting their heterogeneity and varying causes. One such condition, melancholia [previously termed endogenous depression], has long held consistent ascriptions: being genetically weighted, having prominent biological perturbations, evidencing overrepresented clinical features, and showing a greater response to physical therapies than to psychotherapy. As psychiatry strives toward a diagnostic nosology based on genetic, behavioral, and neurobiological criteria, melancholia arguably represents a canonical test case…
Historical failure to identify specific neurobiological correlates of melancholia is consistent with recent advances in cognitive neuroscience that regard the brain as a complex network, whereby psychiatric conditions reflect changes in functional integration rather than perturbations within an isolated region. Large-scale brain networks supporting mood regulation, interoception, and cognition [eg, concentration and attention] are thus likely candidates for furthering understanding of melancholia’s neurobiology…
Conclusions: We position the neurobiological features of the spontaneous dysphoria of melancholia as a weakening of interactions among regions that subserve attention,mood regulation, and interoception. Computational accounts of internally generated thought highlight the importance of a critical homeostatic balance between stable self-regulation and dynamic instability. We propose that our findings reflect a loss of this optimal balance, undermining the adaptive role of interoception.
Lundbeck Press ReleaseSeptember 24, 2014
H. Lundbeck A/S [Lundbeck] and Otsuka Pharmaceutical Co., Ltd. [Otsuka] today announced that the US Food and Drug Administration [FDA] has determined that the New Drug Application [NDA] for brexpiprazole for monotherapy in adult patients with schizophrenia and for adjunctive treatment of major depressive disorder [MDD] in adult patients is sufficiently complete to allow for a substantive review and the NDA is considered filed as of 9 September 2014 [60 days after submission]. The PDUFA date is July 11, 2015…
PsychiatricNewsApril 17, 2015New findings from a phase 3 clinical trial, published today in AJP in Advance, suggest that a recently developed antipsychotic may prove to be one of the next treatments for schizophrenia. Researchers from the Department of Psychiatry at Hofstra North Shore-LIJ School of Medicine conducted a randomized, double-blind, placebo-controlled study with 636 patients with schizophrenia to investigate the efficacy, safety, and tolerability of brexpiprazole—a serotonin-dopamine activity modulator that acts as a partial agonist at serotonin 5-HT1A receptors and dopamine D2 receptors, while antagonizing serotonin 5-HT2A receptors and noradrenaline alpha receptors…
“It is important for clinicians and patients to have a range of treatment options to manage symptoms effectively and safely … as response to therapy can vary greatly from individual to individual and from one medication to the next.” Correll informed Psychiatric News that the Food and Drug Administration will make its final decision about the approval of brexpiprazole for the treatment of schizophrenia as well as major depressive disorder in July…
by Correll CU, Skuban A, Ouyang J, Hobart M, Pfister S, McQuade RD, Nyilas M, Carson WH, Sanchez R, and Eriksson H.American Journal of Psychiatry. 2015 Apr 16 [Epub ahead of print]
OBJECTIVE: The efficacy, safety, and tolerability of brexpiprazole and placebo were compared in adults with acute schizophrenia.METHOD: This was a multicenter, randomized, double-blind, placebo-controlled study. Patients with schizophrenia experiencing an acute exacerbation were randomly assigned to daily brexpiprazole at a dosage of 0.25, 2, or 4 mg or placebo [1:2:2:2] for 6 weeks. Outcomes included change from baseline to week 6 in Positive and Negative Syndrome Scale [PANSS] total score [primary endpoint measure], Clinical Global Impressions Scale [CGI] severity score [key secondary endpoint measure], and other efficacy and tolerability measures.RESULTS: The baseline overall mean PANSS total score was 95.2, and the CGI severity score was 4.9. Study completion rates were 62.2%, 68.1%, and 67.2% for patients in the 0.25-, 2-, and 4-mg brexpiprazole groups, respectively, versus 59.2% in the placebo group. At week 6, compared with placebo, brexpiprazole dosages of 2 and 4 mg produced statistically significantly greater reductions in PANSS total score [treatment differences: -8.72 and -7.64, respectively] and CGI severity score [treatment differences: -0.33 and -0.38]. The most common treatment-emergent adverse event for brexpiprazole was akathisia [2 mg: 4.4%; 4 mg: 7.2%; placebo: 2.2%]. Weight gain with brexpiprazole was moderate [1.45 and 1.28 kg for 2 and 4 mg, respectively, versus 0.42 kg for placebo at week 6]. There were no clinically or statistically significant changes from baseline in lipid and glucose levels and extrapyramidal symptom ratings.CONCLUSIONS: Brexpiprazole at dosages of 2 and 4 mg/day demonstrated statistically significant efficacy compared with placebo and good tolerability for patients with an acute schizophrenia exacerbation.
Dr. Correll has been a consultant and/or advisor to or has received honoraria from Actelion, Alexza, American Academy of Child and Adolescent Psychiatry, Bristol-Myers Squibb, Cephalon, Eli Lilly, Genentech, Gerson Lehrman Group, IntraCellular Therapies, Lundbeck, Medavante, Medscape, Merck, National Institute of Mental Health, Janssen/J&J, Otsuka, Pfizer, ProPhase, Roche, Sunovion, Takeda, Teva, and Vanda; he has received grant support from Bristol-Myers Squibb, Feinstein Institute for Medical Research, Janssen/J&J, National Institute of Mental Health, NARSAD, and Otsuka; and he has been a Data Safety Monitoring Board member for Cephalon, Eli Lilly, Janssen, Lundbeck, Pfizer, Takeda, and Teva.
Funded by Otsuka Pharmaceutical Development & Commercialization, Inc., and H. Lundbeck A/S. Jennifer Stewart, M.Sc. [QXV Communications, Maccles field, U.K.] provided writing support that was funded by Otsuka Pharmaceutical Development & Commercialization, Inc., and H. Lundbeck A/S.
by Kane JM, Skuban, Ouyang, Hobart, Pfister, McQuade, Nyilas, Carson, Sanchez, and Eriksson.Schizophrenia Research. 2015 Feb 12. [Epub ahead of print]
The objective of this study was to evaluate the efficacy, safety and tolerability of brexpiprazole versus placebo in adults with acute schizophrenia. This was a 6-week, multicenter, placebo-controlled double-blind phase 3 study. Patients with acute schizophrenia were randomized to brexpiprazole 1, 2 or 4mg, or placebo [2:3:3:3] once daily. The primary endpoint was changed from baseline at week 6 in Positive and Negative Syndrome Scale [PANSS] total score; the key secondary endpoint was Clinical Global Impressions-Severity [CGI-S] at week 6. Brexpiprazole 4mg showed statistically significant improvement versus placebo [treatment difference: -6.47, p=0.0022] for the primary endpoint. Improvement compared with placebo was also seen for the key secondary endpoint [treatment difference: -0.38, p=0.0015], and on multiple secondary efficacy outcomes. Brexpiprazole 1 and 2mg also showed numerical improvements versus placebo, although p>0.05. The most common treatment-emergent adverse events were headache, insomnia and agitation; incidences of akathisia were lower in the brexpiprazole treatment groups [4.2%-6.5%] versus placebo [7.1%]. Brexpiprazole treatment was associated with moderate weight gain at week 6 [1.23-1.89kg versus 0.35kg for placebo]; there were no clinically relevant changes in laboratory parameters and vital signs. In conclusion, brexpiprazole 4mg is an efficacious and well-tolerated treatment for acute schizophrenia in adults… BEACON trial.
[recolored to match the graph above]
Dr Kane has been a consultant for Amgen, Alkermes, Bristol-Meyers Squibb, Eli Lilly, EnVivo Pharmaceuticals [Forum] Genentech, H. Lundbeck. Intracellular Therapeutics, Janssen Pharmaceutica, Johnson and Johnson, Merck, Novartis, Otsuka, Pierre Fabre, Proteus, Reviva, Roche and Sunovion. Dr Kane has been on the Speakers Bureaus for Bristol-Meyers Squibb, Eli Lilly, Janssen, Genentech and Otsuka, and is a shareholder in MedAvante, Inc.
Ruth Steer, PhD, [QXV Communications, Macclesfield, UK] provided writing support, which was funded by Otsuka Pharmaceutical Development & Commercialization, Inc. [Princeton, USA] and H. Lundbeck A/S [Valby, Denmark].
From the Zucker Hillside Hospital, Glen Oaks, N.Y.; Otsuka Pharmaceutical Development & Commercialization, Princeton, N.J.; and H. Lundbeck A/S, Valby, Copenhagen, Denmark.
I just wrote a three part series on the Academic·Industrial·Complex that was as overly detailed as this post – which is yet another example of what that phrase means. I think I’ve been chasing down the details, looking in vain for something that breaks out of the mold of scientific enterprise being used as a commercially driven advertising platform. And what I find is that the further I look, the worse it gets. I was tempted to say that Brexpiprazole is a weak sister Atypical Antipsychotic with a low Adverse Event profile, but I’m not even sure that’s defensible with just two six week trials. And unmentioned here, they used some idiosyncratic analytic techniques that were unfamiliar to me, but I just didn’t have the libido to look into them further [because there was no primary data to test them with].
In Academic·Industrial·Complex II… I was implying that the $700,000 spent on the study of Seroquel XR® in Borderline patients was a waste of money, but another way of looking at that is that their various trials of Seroquel XR® were overall worth it, because Seroquel® stayed in the Blockbuster range even after the patent expired thanks to Seroquel XR®. That’s an easy mistake to make –  to forget how much money is involved in the commerce of these drugs. Abilify® is currently involved in a similar patent extension scheme, and Johanna Ryan has a first-person blog on RxISK about the pressure to take Abilify®. Even in this era when the pharmaceutical industry has all but abandoned CNS drug development and their patent protections are disappearing, we still feel the rumblings of the now passed golden era of psychopharmacology. The KOL class in academic psychiatry is still playing the only tune they’ve known. And that far right point on the Abilify® chart [on the right] represents the number one best selling drug in the US. The Academic·Industrial·Complex is still very much a major player.
to forget how much money is involved in the commerce of these drugs. Abilify® is currently involved in a similar patent extension scheme, and Johanna Ryan has a first-person blog on RxISK about the pressure to take Abilify®. Even in this era when the pharmaceutical industry has all but abandoned CNS drug development and their patent protections are disappearing, we still feel the rumblings of the now passed golden era of psychopharmacology. The KOL class in academic psychiatry is still playing the only tune they’ve known. And that far right point on the Abilify® chart [on the right] represents the number one best selling drug in the US. The Academic·Industrial·Complex is still very much a major player.
"How many people had been imaged at the CMRR by faculty in the Department of Psychiatry in 1999? Zero. The Department of Psychiatry now images more people in CMRR than all other departments on the campus combined…""I developed an idea to focus our academics on imaging, genetics, and clinical trial research, and the rationale for that being we had one of the greatest imaging centers and that’s what the NIH wanted to do. Genetics were emerging. There hadn’t been a person imaged in CMRR, there hadn’t been a blood drawn for genotyping in the department, and I said – We have to get going in these areas. Both of those areas, I thought, could interact with doing very good clinical trial studies…"
"So, like Dr. [David] Mrazek at Mayo says – "Let’s draw your blood and find out what’s going on in your serotonin or your transporter genes or your metabolic genes and that’ll help us with your treatment. The same is also true for imaging, where we’re now imaging at baseline, giving them medicine, imaging after the study is over, and seeing where does the drug act in the brain…"
"We are now 25th out of 135 medical schools, and that puts us in a good position, but we still have a ways to go. We went from 39th in 1999 to 25th now, and we tripled our NIH funds and expanded the breadth and scope of what we’re able to do. But I’m hoping we’ll be able … to take it up a notch, and move up maybe another ten spots…"
Here’s the part where I’m speculating [but for what it’s worth, I happen to believe this speculation]. In the course of too many training programs and too many fellowships, I’ve worked in or been affiliated with a number of clinical research units and their staff. They have been the most cracker-jack support staff I’ve ever had the pleasure to work with – the crème de la crème, inspired by the possibility of advancing medical science and care – loyal to the researchers as part of the team. But in an Academic·Industrial·Complex, they’re grinding out Clinical Trials that don’t have such lofty goals – "just making a buck." The researchers are less available. For example, Dr. Olson saw Dan Markingson just "four or five times" during his six month’s stint in the CAFE trial, and I don’t know that Dr. Schulz ever met him. My speculation is that the "just making a buck" attitude filters down the ranks – manifesting as a disillusioned "just going through the motions" mentality.
 But whether my speculations are true or not, Drs. Elliot and Turner have opened a window into the world of psychiatry’s Clinical Trials and the whole Academic·Industrial·Complex that goes much further than the tragic case of Dan Markingson, than the Department of Psychiatry, than the State of Minnesota. We need even more than just the Data Transparency we’re seeking. We need Transparency for the whole Clinical Trial process. While I’m personally sensitive to the problem of financing psychiatric education, an area I left reluctantly – no matter what problems the Academic·Industrial·Complex tried to fix, it didn’t justify the obvious lapses in medical ethics that arose out of the solution. Faustian contracts with the Devil rarely do…
But whether my speculations are true or not, Drs. Elliot and Turner have opened a window into the world of psychiatry’s Clinical Trials and the whole Academic·Industrial·Complex that goes much further than the tragic case of Dan Markingson, than the Department of Psychiatry, than the State of Minnesota. We need even more than just the Data Transparency we’re seeking. We need Transparency for the whole Clinical Trial process. While I’m personally sensitive to the problem of financing psychiatric education, an area I left reluctantly – no matter what problems the Academic·Industrial·Complex tried to fix, it didn’t justify the obvious lapses in medical ethics that arose out of the solution. Faustian contracts with the Devil rarely do… Several years ago, I ran across a business magazine cover with a high level AstraZeneca executive being praised for figuring out how to extend the patent life of their blockbuster Seroquel® by getting Seroquel XR® approved. I could never find it again. I still feel the loss because it proved that Seroquel XR® was just a marketing ploy…
New York TimesBy KATIE THOMASAPRIL 17, 2015
Last fall, an article in the American Journal of Psychiatry caught the attention of specialists who treat borderline personality disorder, an intractable condition for which no approved drug treatment exists. The article seemed to offer a glimmer of hope: The antipsychotic drug Seroquel XR® reduced some of the disorder’s worst symptoms in a significant number of patients…
 [see an anachronism…]. Seroquel XR® was just a patent-life extender. Borderline Personality Disorder is a very complex topic and the notion that there will ever be a "right drug" for the condition is about as likely as pigs flying. When I reviewed the article, I located a 2004 Medscape C.M.E. where Dr. Schulz had presented industry-funded studies he’d done with Risperdal®, Zyprexa®, and Seroquel® in patients with Borderline Personality – each one showing some effect; each one written up as if it mattered. I actually saw them as playing the companies off against each other.
[see an anachronism…]. Seroquel XR® was just a patent-life extender. Borderline Personality Disorder is a very complex topic and the notion that there will ever be a "right drug" for the condition is about as likely as pigs flying. When I reviewed the article, I located a 2004 Medscape C.M.E. where Dr. Schulz had presented industry-funded studies he’d done with Risperdal®, Zyprexa®, and Seroquel® in patients with Borderline Personality – each one showing some effect; each one written up as if it mattered. I actually saw them as playing the companies off against each other. In the realm of clinical trials, however, reality is sometimes far messier than the tidy summaries in medical journals. A closer look at the Seroquel XR® study shows just how complicated things can get when a clinical trial involves psychiatric disorders and has its roots in intersecting and sometimes competing interests: a drug company looking to hold onto sales of a best-selling drug, a prominent academic with strong ties to the pharmaceutical industry and a university under fire for failing to protect human study subjects…
In Academic·Industrial·Complex I… we read Dr. Schulz’s plan to finance his department by doing «very good clinical trials» and I suggested two criteria for what that might mean 1. trials that were scientifically justified rather that simply commercials [experimercials] and 2. trials that were well executed. Well this whole series of trials on Atypical Antipsychotics generally flunks number 1. and really outdoes itself with Seroquel XR® [after already studying plain old Seroquel®]. And it flunks number 2. in that the execution here is embarrassingly sloppy. This was a Clinical Trial apparently randomizing all comers, with some outrageous antics along the way, that took five years, cost $700K, involved 100 subjects, and was dolled up and published in the American Journal of Psychiatry as if it said something that mattered. The published results actually made very little sense [see an anachronism…].
Bioethicist Carl Elliot’s main focus is on the conduct of the Clinical Trials in the University of Minnesota’s Department of Psychiatry, and he’s collected an impressive array of examples of dysfunction at multiple levels. The recent investigations by an independent panel appointed by the Association for the Accreditation of Human Research Protection Programs and a report from the Office of the Legislative Auditor not only agreed with Elliot but amplified on his observations. The result was a suspension of all Clinical Trials pending further investigation. Dr. Schulz, Chairman of the Department of Psychiatry stepped down. There is a consensus that the Board of Regents and the University President have little understanding of how to do their jobs. Whistle-blowing nurse Niki Gjere describes an atmosphere of fear, but I was more impressed that everyone from the bottom up seems to be just going through the motions, doing nothing wrong, clueless about the uproar.
While I’m obviously relieved that something is finally going to be done about the situation with the University of Minnesota Clinical Trial program, I don’t think that we’ve yet landed on the most basic ethical dimension of this story. The studies on the table right now are a head to head comparison of three [in-patent at the time] Atypical Antipsychotics in First Episode Schizophrenic cases [CAFE], and a string of Clinical Trials of Atypical Antipsychotics in patients with Borderline Personality Disorder as the drugs arrived on the market. All are studies funded by industry and I believe investigator initiated. I question whether there was any scientific justification for any of these trials at the time they were being conducted. Instead, I would propose that all of them were studies probing for some commercial advantage to the pharmaceutical company paying for the trial, and that a strong motive in proposing these trials in the first place was to finance an Department of Psychiatry.
Every Clinical Trial is human experimentation. We’ve decided that human experimentation is allowed if there have been careful limited trials to assess safety and that the potential outcome of the trial will be of wide benefit to others. There is no reasonable argument that suggests a time release version of Seroquel® will be more effective than the already tested regular Seroquel® in any situation. For that matter, there’s nothing that I know about the Borderline Personality Disorder that suggest any medication will be of lasting benefit. Here’s Dr. Schulz’s slide of the drugs that have already been tried:
And as to CAFE – is it reasonable to recruit patients with a First Episode of Psychosis [likely the biggest event in their lives] into a study that commits them to a year of medication [blinded] in order to use the outcome in some future commercial or sales pitch? I think not.
… R&D is no longer responsible for Seroquel® research – it is now the responsibility of Sales and Marketing. So preclinical research studies aimed at mode of action, although very interesting to both of us, do not translate to marketable messages that will impact sales [at least this is what my commercial colleagues say]. On the other hand, clinical studies that extend the indications for Seroquel® can directly impact sales. With limited budgets, funding of clinical studies will therefore come first.
Now that the case of Dan Markingson’s 2004 suicide is no longer in the realm of unacknowledged tragedy, moved into the public domain by two recent reports villifying the University of Minnesota’s Administration and Clinical Trials program for its handling of the case throughout, we can begin to think about what it all means. The implication in many of the discussions of the case is that the Department of Psychiatry’s Clinical Trials program is more revenue generator than a scientific enterprise, and that Markingson’s case is just the tip of the iceberg large enough to sink the Titanic. And speaking of icebergs, there’s the broader question of the involvement of many other Departments of Psychiatry in churning out industry sponsored [and industry controlled] studies of commercial products with results tipped towards the needs of these sponsor’s products.
In the number of visits I made to come here, learn about what was here, talk with Dean Michael, administrators, faculty, Apostolos, etc., I developed an idea to focus our academics on imaging, genetics, and clinical trial research, and the rationale for that being we had one of the greatest imaging centers and that’s what the NIH wanted to do. Genetics were emerging. There hadn’t been a person imaged in CMRR, there hadn’t been a blood drawn for genotyping in the department, and I said – We have to get going in these areas. Both of those areas, I thought, could interact with doing very good clinical trial studies, and I felt a university department was very important for the faculty involved in what was the latest things happening. My experience at Case, especially working with Herb [Meltzer] and with Joe Calabrese, were that the participation in the clinical trials of new compounds led our faculty to be expert in them, basically the day they were approved. I thought also that by doing very good clinical trials, we could use those results in an interface with imaging and in genetics. So, like Dr. [David] Mrazek at Mayo says – "Let’s draw your blood and find out what’s going on in your serotonin or your transporter genes or your metabolic genes and that’ll help us with your treatment. The same is also true for imaging, where we’re now imaging at baseline, giving them medicine, imaging after the study is over, and seeing where does the drug act in the brain. Or, can we tell who’s going to respond and who’s not going to respond. So the interplay was actually more important than the three items of imaging, genes, and clinical trials.

A difficult and challenging topic, and I think I mentioned earlier that when I came and drew up a strategic plan for our department and worked with Dr. Cerra at the AHC [Academic Health Center] and with Al Michael, I strongly felt that a Department of Psychiatry should be able to be involved in clinical trials to advance treatment and to be very familiar with medicines as they came out. I felt that patients need to be well cared for and highly respected, so with Dr. Cerra and Dr. Michael, I was able to get as part of my package to come here the resources to build the ambulatory research center. And this is in our professional building, it’s 5,000 square feet of space devoted to clinical trials, to assessment for imaging studies, etc. The interview rooms are nice, they have a window, etc. There’s a wonderful reception area and each person who comes to be in the research, is greeted by a person. They have a little area for children to sit if they are going to be in the clinical trial, etc. Exam rooms, conference rooms, the whole thing.
… but psychiatry, boy … front page in the New York Times for even the president of the American Psychiatric Association – grilling, nasty things. His university investigated him thoroughly, and he had done nothing wrong. As a matter of fact, what he had done is he had done exactly what the president of Stanford had asked him to do, Dr. Schatzberg. So, in my impression, looking at this, there probably are some instances of the high-flying industry utilizing academia in ways that was not fully appropriate, that the new guidelines for managing conflicts of interest and improving transparency are very, very appropriate in my mind. I think they, if followed in the way that I think our university has put forward and the way Dr. Cerra has expressed his wish, he, from the first day I met him to now, has said – I want us to be able to collaborate with industry, whether it is pharmaceutical or device, or whatever; but, let’s make it real clear what we’re doing. I think we can move ahead with this. And our conflict of interest policy here at the University is really pretty much that way. Not pretty much, very much – it’s actually as strict as any conflict of interest in the US.
But that’s enough for one post. Carl Elliot and colleague Leigh Turner have felt all along that this case was indicative of a problem that had wide implications. After all, Carl’s first article was entitled "The Deadly Corruption of Clinical Trials", not "The Deadly Corruption of a single Clinical Trial". And yesterday’s New York Times has another case from a Cliinical Trial done in Minnesota [A Drug Trial’s Frayed Promise], obviously pursuing the idea that the Markingson case was just a loud example of something generally rotten in the state of Minnesota.