Posted on Friday 25 July 2014
Chasing the genetics holy grail neglects current patient needPsychology Todayby Allen J. Frances, M.D.July 24, 2014I am a great supporter of mental health research, but worry that it has lost its sense of proportion and is chasing the wrong priorities. The really glamorous stuff consumes almost all of the enormous NIMH budget and now has behind it the huge addition of a $650 million dollar private donation aimed at solving the genetics of mental illness. Neuroscience is an extremely easy sell to Congress and rich philanthropists because it promises so much – that we are on the brink of achieving fundamental breakthroughs in understanding how our genes and brains work [and sometimes don’t work]. But such overpromising ignores the painful lessons of history. The neuroscience and genetic revolutions have been astounding in their technical virtuosity and fascinating in their findings- but to date have not helped a single patient. We have learned a great deal in basic science, but nothing at all that translates to better clinical care.

But there is a cruel paradox when it comes to mental disorders. While we chase the receding holy grail of future basic science breakthrough, we are shamefully neglecting the needs of patients who are suffering right now. It is probably on average worse being a patient with severe mental illness in the US now than it was 150 years ago. It is certainly much worse being a patient with severe mental illness in the US as compared to most European countries. Access to community care and decent housing is deteriorating; hundreds of thousands of psychiatric patients are homeless or in prison; there is little system in the mental health system; and almost all research is strictly biological.
I think the welcome infusion of $650 million dollars would have been much better spent to achieve current tangible results [by funding research and model programs to improve the dreary lives of our patients], rather than betting everything on the future long shot that big bucks can dramatically speed up what will doubtless be decades of painstaking and frustrating genetics research. The neglect of the severely mentally ill is a blight on our society that genetics research will not solve. Its OK to shoot for the stars, but not when we are failing in our day to day responsibility. Less glamour, more compassion.
more compassion.
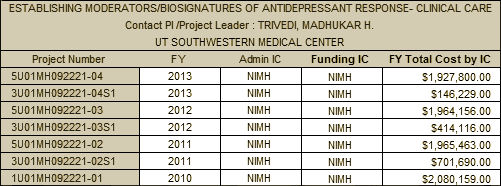
When I read about the $ 650 M commitment to the Stanley Center [$650M gift to Broad seeks to propel psychiatric research], my reaction mirrored Dr. Frances’. I think he’s even more honest than I might have been when he says, "The neuroscience and genetic revolutions have been astounding in their technical virtuosity and fascinating in their findings- but to date have not helped a single patient. We have learned a great deal in basic science, but nothing at all that translates to better clinical care." I might have been too timid to put it quite that strongly, but I sure thought it as soon as I read it. It’s Mr. Stanley’s money and he can choose to do with it whatever he wants to do. He didn’t ask me or Dr. Frances. But if he had…
I guess people think that neuroscience research is like the Manhattan Project, or NASA, or DARPA. If we just throw money and talent at it, it will yield up its secrets. Those were projects where we knew where we were going and a lot about how to get there. The infusions of brainpower and treasure insured that the details would be ironed out and we sped towards the goal. Neuroscience research, particularly genetic neuroscience research, is a horse of a different color. It’s exploratory, a trip into the unknown. We don’t really even know the questions to ask or what we’d do with the answers if we had them. And with much mental illness, we don’t even know if the problems have anything to do with neuroscience, in spite of hearing little else for decades. With Steve Hyman in charge of the Stanley Center and Tom Insel in charge of the NIMH, regrettably, that’s not likely to change.
 It is an anticoagulant that, unlike Warfarin, can’t be reversed if a person has a bleeding episode. Having spent plenty of nights in a former career pumping patients full of Vitamin K to reverse dangerous bleeding, I wondered what one was to do when a person on Pradaxa® slarted bleeding. I had a vision of the little Dutch Boy trying to stop leaks in the Dyke and running out of fingers.
It is an anticoagulant that, unlike Warfarin, can’t be reversed if a person has a bleeding episode. Having spent plenty of nights in a former career pumping patients full of Vitamin K to reverse dangerous bleeding, I wondered what one was to do when a person on Pradaxa® slarted bleeding. I had a vision of the little Dutch Boy trying to stop leaks in the Dyke and running out of fingers. This weeks BMJ hit the ground running on the Pradaxa® story, and good for them. It’s is full of detailed articles documenting the whole mess. There’s plenty of blame to go around: NICE, the FDA, Boehringer Ingelheim, and all physicians involved – including the one that recommended it for my friend, a Habitat for Humanity crew chief who jumps in to do the jobs other volunteers don’t know how to do. I can just hear the phone call that he fell from a ladder [again]. Around that same time he was started on Pradaxa®, a cardiologist from the same practice frowned with disapproval when I declined his recommendation that I take a Statin for my until-recently-normal LDL [although I did get a laugh when I added "I don’t need a Mammogram either"].
This weeks BMJ hit the ground running on the Pradaxa® story, and good for them. It’s is full of detailed articles documenting the whole mess. There’s plenty of blame to go around: NICE, the FDA, Boehringer Ingelheim, and all physicians involved – including the one that recommended it for my friend, a Habitat for Humanity crew chief who jumps in to do the jobs other volunteers don’t know how to do. I can just hear the phone call that he fell from a ladder [again]. Around that same time he was started on Pradaxa®, a cardiologist from the same practice frowned with disapproval when I declined his recommendation that I take a Statin for my until-recently-normal LDL [although I did get a laugh when I added "I don’t need a Mammogram either"].
")
 Scrapings of the rash revealed those little corkscrew Treponema pallidum organisms bending in the middle that I’d only seen in pictures [the organisms that cause Syphilis]. In spite of our starting him on a very low dose of penicillin, he had a Jarisch–Herxheimer reaction [toxicity from the sudden death of the organisms] requiring high doses of steroids. He had been infected by a dalliance with the wife of a ranking officer at a base in another European country [a delicate and touchy point]. He recovered nicely, but unfortunately we were right the first time. On a subsequent liver biopsy, he also had Chronic Active Hepatitis that had been complicated by the Syphilis infection.
Scrapings of the rash revealed those little corkscrew Treponema pallidum organisms bending in the middle that I’d only seen in pictures [the organisms that cause Syphilis]. In spite of our starting him on a very low dose of penicillin, he had a Jarisch–Herxheimer reaction [toxicity from the sudden death of the organisms] requiring high doses of steroids. He had been infected by a dalliance with the wife of a ranking officer at a base in another European country [a delicate and touchy point]. He recovered nicely, but unfortunately we were right the first time. On a subsequent liver biopsy, he also had Chronic Active Hepatitis that had been complicated by the Syphilis infection.