Posted on Sunday 21 February 2016
“To a man with a hammer, everything looks like a nail.”
Whether you attribute the quote to Mark Twain or to Abraham Maslow, the meaning is clear. Which brings me to Aaron Beck, Sigmund Freud, and Tom Insel [OK, actually to Tom Insel]. When a new chairman appeared in my department in the early 1980s, there was a period when we had some interesting discussions. I was a psychoanalytic candidate, was directing a major program in his department [the residency], and was also teaching the major medical school course. We talked about a lot of things in the getting-to-know-you period. He was pretty iconoclastic about almost anything I said, talking excitedly about the future with genetics, biomarkers, PET Scanners, and psychopharmacology. When our honeymoon was over, I was moving on, but I never forgot those talks – because I’ve heard them in one form or another from one person or another for the ensuing decades. The classic version came from Dr. Insel’s Psychiatry-as-Clinical-Neuroscience meme where he literally plotted out our future based on the same new technologies my new chairman had outlined twenty years earlier. If there were ever a man with a hammer, it was Tom Insel:
In 2009, Dr. Insel started writing his Director blogs, many of which were about even newer technologies and the progress they promised. About that same time, we began to hear about something new:
“Can we develop a clinically useful diagnostic system based on neuroscience and genetics? Not yet. But, in the spirit of beginning a long journey, NIMH is taking its first step with the Research Domain Criteria [RDoC] project. RDoC makes no assumptions about current categories”…“Our vision is a new classification with high reliability and validity based on a deep understanding of the neural basis of mental disorders.”Re-Thinking Classification of Mental Disorders |February 1, 2010|
Then just prior to the release of the DSM-5 in 2013, he announced that the RDoC was replacing it as the official diagnostic system of the NIMH [Transforming Diagnosis]. Time passed, and in August of last year, he returned from a tour of high-tech companies, enthusiastic about what he’d seen in this travels:
“While the focus of wearable technology and online apps has thus far mostly been for managing heart disease and diabetes, the tech approach may be best suited for mental health. The biomarkers for depression and psychosis and post-traumatic stress disorder are likely to be objective measures of cognition and behavior, which can be collected by smartphones. Some of our most effective interventions are psychosocial treatments that can be delivered or extended by smartphones and tablets. Most important, the sensors and the interventions can be integrated into a closed loop so that care is continuous and iterative. Increasing symptoms, suicidal impulses, and paranoid thoughts lead immediately to an intervention.”Look who is getting into mental health research |August 31, 2015|
We didn’t yet know it, but his summer tour of the high tech world was also a job search, and within a few weeks, he announced he was stepping down [ambivalence…] to sign on with Google. In the multiple interviews about why he was leaving, this one sounded close to the center to me:
Why did you leave the National Institute of Mental Health to work for Google?I have to confess that after giving heart and soul to mental-health problems over the last 13 years working in government, I have not seen any improvement for either morbidity or mortality for serious mental illness – so I’m ready to try a different approach. If it means using the tools available in the private sector, let’s go for it.Are you saying Google is a better place to do mental-health research than the NIMH?I wouldn’t quite put it that way, but I don’t think complicated problems like early detection of psychosis or finding ways to get more people with depression into optimal care are ever going to be solved solely by government or the private sector, or through philanthropy. Five years ago, the NIMH launched a big project to transform diagnosis. But did we have the analytical firepower to do that? No. If anybody has it, companies like IBM, Apple or Google do – those kinds of high-powered tech engines…Brain expert: Why I jumped ship to Google |Nov 4, 2015|
You could read his comments as blaming, like the NIMH let him down – didn’t live up to his expectations – didn’t provide him with "the analytical firepower" he needed to develop his RDoC. For most of us, all we know is what the RDoC isn’t, but only know about what it is in the vaguest of general terms. So we can’t possibly have a clue what he’s talking about, how the absence of "the analytical firepower" let him down. Is he saying that the RDoC is a bust too, like the DSM-5? It has seemed to me that the question at hand is pretty clear. Is the RDoC an Insel-ism, a part of his clinical neuroscience monomania? something that needs to exit along with him and his hammer? already an anachronism before we even got to know it? Or is it a viable and valuable legacy that ought it be pursued?
Somebody in the NIMH must’ve known some of us were thinking these thoughts, because this month’s issue of Psychophysiology is devoted entirely to the RDoC. It starts with a couple of articles explaining the RDoC and how it came to be in existence, followed by a number of investigators using this new system. The whole issue is freely avaliable on-line. So I guess we can’t complain that they haven’t really told us what’s going on. The ball’s in our court now, and here are the links:
 The Physicians Desk Reference [PDR] has grown since it was introduced in 1947, the year I started the first grade. It was still pretty thin when I started medical school in 1963, just a year after the Kefauver-Harris Drug Efficacy Act passed in the aftermath of the Thalidamide affair. The Act charged the FDA with certifying efficacy by at least two well conducted clinical trials in addition to its traditional safety evaluations.
The Physicians Desk Reference [PDR] has grown since it was introduced in 1947, the year I started the first grade. It was still pretty thin when I started medical school in 1963, just a year after the Kefauver-Harris Drug Efficacy Act passed in the aftermath of the Thalidamide affair. The Act charged the FDA with certifying efficacy by at least two well conducted clinical trials in addition to its traditional safety evaluations.  Then in the 1980s, again in response to pressure, this time from the HIV victims, there was a movement to publicly register Clinical Trials. Those efforts culminated in the FDA Modernization act of 1997 that created clinicaltrials.gov – a public registry. It was originally conceived as placing parentheses around a trial [a registration database up front and reporting database when completed], but only the registration actually caught on. The post-completion reporting database cupboard is bare, and has been, even in situations where reporting is mandatory within one year, like in government funded trials. They just didn’t do it. My accounting only covers high points, but it gives the flavor of how things have gone – a chess game that doesn’t seem to end. And a PDR that just keeps on growing – filling with drugs some of whose efficacy and safety have been exaggerated…
Then in the 1980s, again in response to pressure, this time from the HIV victims, there was a movement to publicly register Clinical Trials. Those efforts culminated in the FDA Modernization act of 1997 that created clinicaltrials.gov – a public registry. It was originally conceived as placing parentheses around a trial [a registration database up front and reporting database when completed], but only the registration actually caught on. The post-completion reporting database cupboard is bare, and has been, even in situations where reporting is mandatory within one year, like in government funded trials. They just didn’t do it. My accounting only covers high points, but it gives the flavor of how things have gone – a chess game that doesn’t seem to end. And a PDR that just keeps on growing – filling with drugs some of whose efficacy and safety have been exaggerated… 
 So as the world of drug testing has become increasingly distant from academic influence and control, why are the academic authors still involved? My guess is that they bring the aura of an academic standard and a medical ethic to the trials, and, of course, serve as a ticket into the traditional academic journals. To my mind, this meta-analysis is just further evidence that that influence is simply a mirage. There are many other more effective ways to insure that product testing is on the up and up. The academic community would be more usefully engaged in vetting the data that these trials produce, disconnected from the manufacturers.
So as the world of drug testing has become increasingly distant from academic influence and control, why are the academic authors still involved? My guess is that they bring the aura of an academic standard and a medical ethic to the trials, and, of course, serve as a ticket into the traditional academic journals. To my mind, this meta-analysis is just further evidence that that influence is simply a mirage. There are many other more effective ways to insure that product testing is on the up and up. The academic community would be more usefully engaged in vetting the data that these trials produce, disconnected from the manufacturers.
 I was writing about Harlan Krumholtz’s paper in the BMJ, and took a break to watch The Blacklist episode I missed [on the DVR]. About two-thirds through, I was fast-forwarding through the commercials but I was stopped in my tracks as a logo I recognized flashed by – Rexulti®. So I watched the ad and found myself screaming at the television set. In case you forgot about it, it’s the Abilify clone, the one that had two articles in succession in the JCP that were cut and paste copies, only one academic author [KOL Michael Thase], and was approved by the FDA as an adjunct for Treatment Resistant Depression, in spite of not making it without jury-rigging the results. For review:
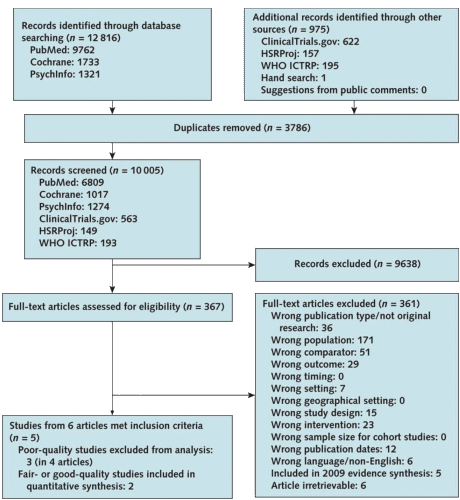
I was writing about Harlan Krumholtz’s paper in the BMJ, and took a break to watch The Blacklist episode I missed [on the DVR]. About two-thirds through, I was fast-forwarding through the commercials but I was stopped in my tracks as a logo I recognized flashed by – Rexulti®. So I watched the ad and found myself screaming at the television set. In case you forgot about it, it’s the Abilify clone, the one that had two articles in succession in the JCP that were cut and paste copies, only one academic author [KOL Michael Thase], and was approved by the FDA as an adjunct for Treatment Resistant Depression, in spite of not making it without jury-rigging the results. For review:  I’ve read all the studies reviewed in 2009 and this current version. There’s not even a hint of a rational reason to recommend a preventive intervention in adolescent depression, and what these USPSTF papers conclude is as much bull-shit as some of the papers themselves. I’ve read a lot of the papers in the adult articles too. Same deal. So when I think back on my soldier days in the early 1970s, I wish I’d had my present mind and spoke it. Our Base Commander wasn’t thinking about his troops’ health. He was thinking about how they looked on inspections, or about being strong on the "regs," or about getting that star he wanted on his epaulets. And the reason he wasn’t going to get the star was widely known by all – his affinity for bourbon – which made his subsequent campaign even sillier.
I’ve read all the studies reviewed in 2009 and this current version. There’s not even a hint of a rational reason to recommend a preventive intervention in adolescent depression, and what these USPSTF papers conclude is as much bull-shit as some of the papers themselves. I’ve read a lot of the papers in the adult articles too. Same deal. So when I think back on my soldier days in the early 1970s, I wish I’d had my present mind and spoke it. Our Base Commander wasn’t thinking about his troops’ health. He was thinking about how they looked on inspections, or about being strong on the "regs," or about getting that star he wanted on his epaulets. And the reason he wasn’t going to get the star was widely known by all – his affinity for bourbon – which made his subsequent campaign even sillier.